We live in a time where an intimate question about identity has transformed into a public battlefield. The issue of transgender teenagers — and how society navigates it — has become a symbolic flashpoint in the global culture war.
At the extreme ends of the spectrum, fierce convictions collide. Some speak of a ‘contagious ideology,’ a social fad sweeping young people into irrevocable choices. Others see it as a life-saving recognition of suppressed identities — a necessary correction to centuries of societal denial.
And then there is the large middle group. People who wonder what is true, what is exaggerated, and what is being left unsaid. Those who don’t buy into the rhetoric of panic or pathos, but who crave clarity. Because behind all the shouting lies real confusion — and genuine questions about young lives in development.
So, what is going on?
- Is it true that an increasing number of teenagers are identifying as transgender?
- What does so-called gender-affirming care actually entail?
- Does it have a proven effect — and for whom?
- And why are countries like Sweden, Finland, and the United Kingdom now putting the brakes on treatments that were presented as progressive just a few years ago?
These are the questions we explore in this article.

Sex and Transgender Teenagers
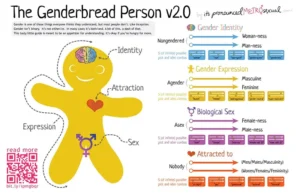
For the vast majority of people, biological sex is straightforward. Most bodies are born with characteristics we categorize as male or female. While intersex variations exist, they remain exceptional.
In biological terms, it is simple. Individuals with XX chromosomes typically develop ovaries and breasts — and are categorized as female. XY chromosomes direct development toward testicles and testosterone. What appears relatively clear at a medical level quickly becomes a different story at a psychological level.
Gender identity — how someone feels and identifies internally — is anything but straightforward. It is not a matter of chromosomes or organs, but of experience, meaning, and interpretation. This makes it harder to capture in fixed definitions. Psychologists suspect it arises from an interplay of genetic predisposition, physical factors, social experiences, and cultural expectations. In short: it is complex — and often confusing, even for the individual themselves.

Transgender and Gender Dysphoria
When the inner experience of gender stands at odds with the sex assigned at birth, we use the term transgender. Those who identify with their assigned sex are generally called ‘cisgender’ — though that label speaks more to classification than to identity itself.
For some transgender individuals, this discrepancy is overwhelming. It feels like living in a body that tells a different story than the one you feel inside. Not everyone finds this problematic, but those who do may develop gender dysphoria — a recognized psychological syndrome that can be accompanied by depression, anxiety, and deep alienation from one’s own body.
The debate over language also plays a role. Many within the transgender community prefer terms like “experienced gender” over “biological sex” — not out of semantic hypersensitivity, but because the difference between what you *are* and what was *assigned* to you is crucial to their narrative. And language, however imperfect, is often the first tool people use to shape their inner worlds.
Being transgender is not a modern invention. In myths, religions, and cultures, we find traces of people who did not feel at home in the strict division of male or female for centuries. It is not a mental disorder in itself, but a less common variant in the spectrum of human development. And perhaps… a mirror for our persistent tendency toward binary thinking.
Let me state one thing clearly: the idea of a “normal” human development is debatable, to say the least. Have you ever met a normal person? Neither have I. And perhaps that is the core of the problem — that we constantly try to capture something erratic and individual within fixed models and diagnoses.

The phenomenon of being transgender is not a 21st-century trend. In various cultures — such as the hijra in India or the kathoey in Thailand — social roles for people outside the male-female duality have existed for generations. But while some societies offered space for these third forms of gender, in other contexts, transgender people have been systematically marginalized, ridiculed, or even criminalized.
These patterns continue today. In countries like Indonesia and Nigeria, being transgender is legally prohibited. And even in relatively tolerant societies, the social reality remains harsh: violence, exclusion, and a constant pressure to fit into a binary mold.
Gender-Affirming Treatments and Transgender Self-Identification
Starting in the 1970s, the medical world began to intervene — with the intent to alleviate psychological suffering in transgender individuals. Remarkably, it was Dutch doctors who led the way in this field. This isn’t a medical history lecture, so we’ll skip the detours, but to understand today’s debate, it’s important to look at how psychiatry currently defines gender dysphoria.
In the DSM-5-TR, the current standard for diagnosing mental disorders, gender dysphoria in children is described as a persistent and clear discrepancy between experienced gender and birth sex. This discrepancy must last at least six months, be accompanied by significant stress, and meet several additional criteria, such as a strong desire to be the other gender or an aversion to physical characteristics associated with the assigned sex.
In other words: it must be tangible, long-lasting, and impactful enough to justify a diagnosis.
What do the numbers actually say? Across the world, various studies and policy shifts are visible — sometimes affirming, sometimes retreating. The picture is fragmented, but not without patterns.
| Country | Percentage of Transgender Identification | Notable Findings |
|---|---|---|
| United Kingdom | 0.5% | One in five transgender students reports sexual violence during a date. One in three has attempted to take their own life. |
| United States | 0.6% | Transgender students face a suicide attempt risk three times higher than cisgender girls. |
| Canada | 0.19% transgender 0.15% non-binary |
The proportion is significantly higher among teenagers than adults — a trend that raises questions. |
| Finland | – | Since 2020, the minimum age for gender-affirming surgeries has been raised from 18 to 25. |
| United Kingdom | – | Children under 16 no longer receive hormone treatment, due to caution regarding effectiveness and risks. |
What stands out is that while identification figures often seem small, the psychological impact is anything but marginal — especially among the youth.
The State of Affairs in the Netherlands: Anno 2025
📊 Numbers and Percentages
-
Transgender Adults: Approximately 1% of the Dutch population aged 15 and older identifies as transgender. This equates to about 151,000 people, including transgender men, women, and non-binary individuals, according to an analysis by the CBS on the size of the LGBTQIA+ community.
-
Transgender Youth: A long-term study from UMCG shows that at age 11, 11% of youth expressed a desire to be the opposite sex, but this decreases to 4% by age 25. Only 0.1% of youth consistently maintained this desire. You can read more about this at the Netherlands Youth Institute (NJi).
🏥 Healthcare and Waitlists
-
Number of Applications: The number of young people applying for transgender care continues to grow. In 2021, 1,855 youth under 18 were on the waitlist for an intake, compared to 1,179 the previous year. See the full article from NOS on rising applications and waitlists.
-
Wait Times: The average wait time for an initial consultation in transgender care currently stands at 36 weeks, as noted in the same NOS article.
🧠 Psychological Well-being
-
Gender Questioning Often Decreases: As mentioned in the UMCG study, gender questioning among youth is often temporary. These findings are summarized on the NJi website.
-
Correlation with Mental Health Issues: Youth who express a desire to be the opposite sex more frequently experience psychological problems such as anxiety or negative self-image. This is also discussed in the Netherlands Youth Institute publication.
📉 Acceptance and Discrimination
-
Decline in School Acceptance: The number of young people with negative views toward transgender persons has increased: from 13% in 2021 to 25% in 2023, according to research by Transgender Network Netherlands.
-
Violence and Bullying: Among openly transgender students, 43% report facing verbal violence, and 20% physical violence. More on this can be found in Gendi’s overview of facts and figures regarding LGBTI youth.
Transgender Self-Identification
What happens when young people begin to identify themselves differently from what is written on their birth certificate? Self-identification as transgender is not new, but its visibility is increasing — and that raises questions.
In Western countries, about half a percent of the population indicates they do not identify with their birth sex. In the 2021 UK census, 0.5 percent of respondents over 16 stated their gender differed from what was officially registered. In the United States, this percentage was slightly higher at 0.6 percent, according to Census Bureau data.
Canada reported in 2021 that 0.19 percent of the population identified as transgender and 0.15 percent as non-binary — though the ratio among youth appears significantly higher than among adults. This difference is intriguing and forms the starting point for a broader discussion on societal change and psychological development.
A large 2017 survey of 125,000 American high school students showed that transgender youth not only experience dating violence more often (over 20%), but approximately one-third have attempted suicide. That is more than three times higher than among cisgender girls — a statistic that demands serious reflection.
In response to these figures, some countries have opted for so-called gender-affirming care: hormone therapy, puberty blockers, or — in rare cases — surgical interventions. But this approach is not without controversy. Finland raised the minimum age for surgeries from 18 to 25 in 2020, and the United Kingdom decided to no longer offer hormone treatment to children under 16.
What stands out is not just the growth of self-identification, but the divergent ways in which societies are now reacting — balancing between protection and restraint, recognition and regulation.

More Teenagers Reporting Gender Dysphoria
Research from the Williams Institute (UCLA) shows that 1.4 percent of American youth aged 13 to 17 identify as transgender. That is more than twice the rate among adults. And while the percentage among adults has remained stable for years, it nearly doubled among teenagers between 2016 and 2021.
This is a remarkable increase — one that cannot be viewed separately from broader cultural, psychological, and social dynamics. Whether this rise reflects greater freedom or greater confusion remains an open question for now.
The number of gender clinics in the United States treating youth has exploded over the past fifteen years — from virtually zero to over one hundred. An impressive figure, but like the wrinkles on a person’s forehead, growth in itself says nothing about causes. Correlation is still not proof of causality — though it certainly raises questions.
According to Komodo Health data (commissioned by Reuters), the number of insured children aged 6 to 17 with a diagnosis of gender dysphoria in the US rose from 15,000 in 2017 to 42,000 in 2021. A doubling, even a tripling — depending on how you calculate. About six thousand of these children used puberty blockers or underwent hormone therapy. It is assumed that actual numbers are slightly higher, but structurally, that changes little of the big picture.
The Total Number of Children Using Medication for Gender Dysphoria is Small
Put those numbers into perspective: it concerns about three out of every ten thousand children — in a group of about 25 million American youth. A small group, indeed, but one that evokes a disproportionate amount of societal attention and controversy.
And it is not a uniquely American phenomenon. In the United Kingdom, referrals to the Gender Identity Development Service increased twenty-fold between 2011 and 2020. Similar increases were recorded in Canada, Sweden — and closer to home, in the Netherlands and Spain.
The Netherlands, Spain, the UK, Canada, and Sweden
What is striking is that the majority of new reports come from children classified as female at birth but identifying as male. A notable shift, as earlier generations showed a more even distribution — or even a slight overrepresentation of boys. The figures are widely shared, but there is deep division regarding their interpretation.
In 2018, American physician Lisa Littman published a controversial paper describing how many of these girls suddenly developed gender dysphoria during adolescence without prior childhood signals. She introduced the term “Rapid Onset Gender Dysphoria” (ROGD) and suggested it might be a socially mediated phenomenon. Through social media or contact with peers, these girls supposedly formed the idea that gender transition would solve their problems.
The hypothesis hit like a bomb. On the surface, it sounds logical: adolescents — and girls in particular — struggle with psychological issues like anxiety and depression at above-average rates. Those who feel unhappy search for explanations — and for solutions.
Littman further hypothesized that girls are more susceptible to social influence than boys, though she admits that convincing evidence for this is lacking. The idea of social contagion therefore remains a theory for now — intriguing, but insufficiently proven.

Insufficient Evidence For or Against Rapid Onset Gender Dysphoria
Littman’s hypothesis, however provocative, faced heavy criticism. Not so much for her intent, but for her research design. The data used came from parents active on forums critical of youth transgender self-identification. The sample was far from representative.
Littman herself calls her work a “descriptive, exploratory study.” She made no hard claims but outlined patterns in what parents reported. What that means for the broader phenomenon remains speculative.
Remarkably, the ‘refutation’ of it also faced criticism. A paper appearing in August of last year claimed to have proof that the “rapid onset” phenomenon does not exist. But this study was also under fire — due to ambiguous survey questions and creative interpretations of data. The irony: both the theory and the counter-reaction prove to be methodologically fragile.
The conclusion? There is currently no conclusive scientific evidence for or against the existence of a sudden onset of gender dysphoria in adolescents. What does persist are anecdotal observations from doctors and clinic staff — impressions that suggest something is occurring but cannot yet be hard-proven.
Increase of Gender Dysphoria in Girls
What is, however, indisputable from the data is the sharp increase in the number of girls reporting gender dysphoria. And it is this shift — not the surrounding hypothesis — that demands further explanation.
Gender-Affirming Care and Mental Health Problems
Doctors are flagging another emerging concern: many of the girls reporting gender dysphoria today also have other psychological diagnoses or struggles. Think of anxiety disorders, trauma, or neurodiverse traits. This raises the question of whether the gender dysphoria stands alone — or is part of a broader psychological tension.
The standard treatment path is called ‘gender-affirming care.’ It typically begins with social transition: a different name, different pronouns, an adjusted clothing style, and joining peer groups that match the experienced gender. The idea is to provide space for exploration without immediate medical intervention.
Puberty Blockers and Hormone Therapy
Around age ten — sometimes earlier — medical choices come into play. This is when puberty blockers are utilized: medications that temporarily halt the development of secondary sexual characteristics. No breast growth, no beard growth, no menstruation. Put on pause, as it is often presented. But what does that mean psychologically at that age?
The drugs are administered via injections (monthly or every three months) or implants that must be replaced annually. The idea is to buy time: creating space for reflection before irreversible physical changes occur. Yet, it rarely feels like a pause. You are standing still while everyone around you is accelerating — an experience that, for some, triggers new stress.
If the trajectory continues, youth typically start hormone therapy around age fifteen. For boys, this means estrogen and a testosterone blocker; for girls, the reverse. Physical changes then begin — and with them, the question of what is reversible and what is not.
Surgery and Costs
Those who choose medical transition rarely stop halfway. Research shows that the vast majority of youth who start with puberty blockers — as high as 95 percent in the Netherlands — eventually proceed to hormone therapy. Some also choose surgeries later in life, such as breast removal (top surgery), genital reconstruction (bottom surgery), or the removal of internal reproductive organs.
Surgeries on children, however, are virtually unheard of. They also remain rare among teenagers. Most procedures take place in (young) adulthood, when the body is fully developed and psychological stability can be better assessed.
But the costs are substantial, especially in countries without public healthcare. In the US, the monthly cost for hormone therapy ranges between 100 and 200 dollars, excluding consultations and psychological support. Top surgery — usually removing or constructing breasts — starts at 3,000 to 10,000 dollars. Genital surgery is much higher: averaging around 25,000 dollars.
And even then: those are just the direct surgical costs. Recovery time, aftercare, psychological counseling, and hormonal follow-up quickly add up. According to experience reports, the total cost for a full medical transition path can exceed 100,000 dollars — even with insurance.
And let’s be honest about the terminology. “Top surgery” and “bottom surgery” sound friendly, but they involve the removal of body parts that do not grow back. There is no Ctrl-Z. And that fact demands deep consideration, not simplified slogans.
Effectiveness of Puberty Blockers
One would hope that such invasive and costly treatments are at least effective. But that is — to put it mildly — not self-evident. Puberty blockers do what their name suggests: they inhibit puberty. But the side effects are significant: weight gain, headaches, stunted growth, and decreased bone density.
Officially, they are called “reversible” — the idea being that development simply resumes once you stop. But this is a simplification that is increasingly under fire. Long-term studies show that bone density in many users does not fully recover, which increases the risk of fractures later in life.
Other studies signal increased risks of heart problems, underdevelopment of sex organs, and fertility issues. But here too, the samples are small, the results preliminary, and often internally contradictory.
Added to this is a social-psychological complication. Those who do not go through puberty while their peers do become socially isolated — or feel like an outsider in their own body. The waiting then becomes not a relief, but an extension of the confusion.
In 2016, the US FDA decided to require manufacturers of puberty blockers to add a warning: reports had come in of children developing suicidal thoughts after using the medication.
Limited Effectiveness of Puberty Blockers
The question remains: do puberty blockers actually help youth with gender dysphoria psychologically? The evidence is razor-thin. Some studies show a slight decrease in suicidal thoughts, but they lacked a control group — meaning it could have been the attention and care itself that brought temporary relief.
Other studies showed that for youth with severe, persistent gender dysphoria, the use of puberty blockers brought no significant improvement in body image or the tendency toward self-harm.
And that is perhaps the most difficult conclusion so far: we are facing a medical path with lasting consequences but limited certainty regarding the outcomes.
In 2020, the British National Institute for Health published a systematic literature review on the effect of puberty blockers. Their conclusion was hardly reassuring: the quality of existing research was rated as “very low,” and the observed changes between baseline and final measurements were minimal — both in terms of gender dysphoria and mental health or psychosocial impact.
Puberty Blockers and Hormone Therapy for Transgender Youth: What Do We Know?
The researchers added a striking quote: “Studies that found differences in outcomes may show changes that are clinically questionable, or arise from confounding factors, bias, or chance.” In other words: even where something seems to work, it is questionable whether it actually works.
Then there is hormone therapy — where the body is artificially shaped toward the characteristics of the chosen gender. Usually, this process begins between ages 16 and 18. Certain changes are reversible if one stops: skin texture, muscle mass, fat distribution. But others are not.
Voice changes, breast formation, male-pattern baldness, or a visible Adam’s apple do not reverse. And once your hair is gone, estrogen unfortunately won’t bring it back — however much we might want to believe otherwise. The long-term effects on fertility remain uncertain for now, though concerns about permanent damage to reproductive organs are growing.
But Does the Well-being of Transgender People Benefit?
A recent American study followed 315 transgender and non-binary youth, aged 12 to 20, for two years. The researchers reported statistically significant improvements in ‘appearance congruence’ (the feeling that your appearance matches your gender), positive affect, and general life satisfaction. Anxiety and depression scores also slightly decreased.
But here is the nuance: life satisfaction increased by an average of 2.3 points per year — on a scale of 100. Depression scores fell by 1.3 points on a scale of 63. Statistically significant, yes. But clinically relevant? That is another matter.
And then there is something else noteworthy. These slight improvements were only seen in youth assigned female at birth. In the group born as boys, researchers saw no statistically relevant decrease in anxiety, depression, or dissatisfaction. A detail that was missing from the study’s abstract but could be found in the underlying data.
Maybe That is the Right Explanation, or Maybe Not
The authors speculated that this difference might be because trans girls — classified as boys at birth — need more time before hormonal changes become visible. Breast growth is slow, especially compared to the effect of testosterone in trans boys.
Furthermore, they state, social acceptance differs greatly between trans men and trans women. The context in which youth experience their transition likely influences the outcome more than the hormones themselves. Which is unsurprising, considering mental health is rarely independent of social treatment.
The researchers also referred to a 2019 meta-analysis which found that testosterone treatment can significantly reduce depressive symptoms in biological men. The question then is: does the effect come from the gender transition — or simply from the physiological action of the hormone?
So maybe it was the hormones. Or maybe something else.
Jesse Singal, a journalist who has been critical of youth transgender care, points out that the variables examined in the study did not match what was pre-registered in the research protocol. This means the researchers — consciously or unconsciously — had room to select which results they presented after the fact. Not direct fraud, but it certainly undermines the reliability of the conclusions.
The Journal Pediatrics
Another frequently cited study, published in the prominent journal Pediatrics (2022), followed approximately 100 American youth who were transgender or non-binary. Or that was the plan, at least. By the end of the study, only 64 participants remained.
Or rather: they tried. But by the end of the study, only 64 participants were left — a group so small that any conclusion must be read with extreme caution.
About two-thirds of these youth started puberty blockers or hormone therapy during the study. The rest — a meager control group — did not. The researchers reported that treated youth had a 60% lower chance of depression and a 73% lower chance of suicidal thoughts. However, no difference was found for anxiety symptoms.
Sounds promising? Here is the footnote. The psychological health of the treated group didn’t necessarily improve; what actually happened was that the untreated group declined. The control group ultimately consisted of only seven people — a number with almost zero statistical power. The difference, then, perhaps says more about who was left behind than about who was helped.

Summary
What stands out in all the data: the increase in young people identifying as transgender is not only real, but substantial. And the composition of that group has changed. Increasingly, it is girls — or rather: youth classified as female at birth — who are applying with gender dysphoria. And a striking number of them also face other psychological vulnerabilities.
The evidence that puberty blockers or hormone therapy actually help these youth is meager. The studies are small, the results contradictory, and the risks are non-negligible. Side effects are real. Long-term consequences are largely unknown.
What exactly is happening? No one knows for sure. What does seem plausible is that two movements are occurring simultaneously: youth feel safer being openly trans — and some think they are trans because the narrative is everywhere. Both scenarios can be true. It is the refusal to admit that which clouds the conversation.
Anyone claiming only one of these possibilities exists is pushing an agenda. Not science. Not care. Not space for doubt — even though that doubt is exactly what is needed right now.
And that is precisely why countries like Sweden, Finland, and the United Kingdom are adjusting their approach. Not because they have become less tolerant, but because they realize that restraint can be a form of protection. Sometimes, the greater risk… is wanting to help a bit too fast.
So: how do you separate the real stories from the assumptions? How do you see the difference between a cry for help and a misplaced hope? As long as we don’t have a clear answer to that, caution is not coldness. It is a moral duty.
Perhaps you are the parent of a child in this age group yourself. Or perhaps you are transgender and view this data differently. Either way — this discussion deserves more than just a for-or-against. It requires people who dare to listen without immediate judgment.
Sources Consulted:
- CBS: How many LGBTQIA persons does the Netherlands have? – Estimate of the number of LGBTQIA persons in the Netherlands, including transgender adults.
- NJi: Gender questioning decreases with age – Research on the decline of gender questioning in youth as they get older.
- NJi: More youth seeking transgender care – Increase in applications for transgender care and the impact on waitlists.
- Transgender Network Netherlands: Acceptance of transgender youth in schools plummeting – Deterioration of acceptance of transgender youth in education.
- Gendi: Facts & Figures about LGBTI+ – Statistics on bullying and violence against transgender youth.
- NOS: Increase of youth in transgender care leads to even longer waitlists – Article on rising applications and wait times in transgender care.
- Leibowitz, S., & Vries, A. (2016). Gender dysphoria in adolescence. International Review of Psychiatry, 28, 21 – 35. – Discusses gender dysphoria in adolescence and its psychological implications.
- Cohen-Kettenis, P., & Klink, D. (2015). Adolescents with gender dysphoria. Best practice & research. Clinical endocrinology & metabolism, 29 3, 485-95. – Covers best practices and research on gender dysphoria in adolescents from a clinical endocrinology perspective.
- Rosenthal, S. (2014). Approach to the patient: transgender youth: endocrine considerations. The Journal of clinical endocrinology and metabolism, 99 12, 4379-89. – Guidelines and considerations for endocrinological care for transgender youth.
Related Articles





Frequently Asked Questions
What is gender dysphoria?
Gender dysphoria is a recognized psychological condition where an individual experiences persistent and significant stress because their inner experienced gender does not match the sex assigned at birth.
Why is the number of transgender teenagers rising?
The increase seems to stem partly from greater openness and social acceptance, allowing youth to feel safer expressing themselves. At the same time, there are concerns about potential influences from social media and group dynamics, especially among vulnerable teenagers.
What does gender-affirming care entail?
Gender-affirming care includes a combination of social, medical, and psychological support to align an individual’s body or living environment with their experienced gender identity. This can range from name changes to puberty blockers or hormone therapy.
Are puberty blockers and hormone therapy effective?
Medical effects are varied and have not yet been sufficiently studied long-term. Some youth report temporary relief from psychological symptoms, but structural improvements in well-being have not yet been convincingly proven scientifically.
Why are some countries restricting gender-affirming care for children?
Countries like Sweden, Finland, and the UK are choosing restraint due to uncertainty about long-term effects, potential risks, and the lack of unambiguous evidence that these treatments structurally contribute to the mental well-being of youth.